mRNA Vaccines Put You at Risk for Acute Coronary Syndrome
STORY-AT-A-GLANCE
- Using the PULS cardiac test, researchers have found Pfizer and Moderna mRNA COVID shots dramatically increase biomarkers associated with thrombosis, cardiomyopathy and other vascular events following vaccination
- Pre- and post-injection PULS tests for 566 patients were compared. On average, their PULS scores went from an 11% five-year risk for acute coronary syndrome, to a more than double, 25%, five-year risk
- Those who got the injection for fear that COVID-19 might adversely affect their heart now face the grim reality that they’ve exchanged a potential risk for a more certain one
- Another paper details how the mRNA shot can cause thrombocytopenia (low platelet count) through a mechanism that involves the activation of platelets by antibodies against the spike protein (anti-spike antibodies)
- A mystery that remains to be solved is why only certain people with antibodies to the spike protein (anti-spike antibodies) go on to develop symptoms of platelet activation and thrombocytopenia. One hypothesis is that only a subset of the anti-spike antibodies formed after vaccination can activate platelets and cause thrombocytopenia
In a November 21, 2021, tweet, cardiologist Dr. Aseem Malhotra writes:1
“Extraordinary, disturbing, upsetting. We now have evidence of a plausible biological mechanism of how mRNA vaccine may be contributing to increased cardiac events. The abstract is published in the highest impact cardiology journal so we must take these findings very seriously.”
The abstract he’s talking about is “mRNA COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and ACS Risk as Measured by the PULS Cardiac Test: A Warning,” published in the November 16, 2021, issue of the journal Circulation.2 (ACS is Acute Coronary Syndrome).
Cardiac Risk Warning
The PULS (Protein Unstable Lesion Signature) cardiac test3 is a simple blood test that detects unstable cardiac lesion rupture, one of the leading causes of heart attacks. As noted by the authors of that paper, this is “a clinically validated measurement of multiple protein biomarkers,” which include:
- IL-16, a proinflammatory cytokine
- Soluble Fas, an inducer of apoptosis
- Hepatocyte growth factor (HGF), a marker for chemotaxis of T-cells into epithelium and cardiac tissue
These and several other proteins are indicative of your immune system’s response to arterial injuries that can result in cardiac lesions. These lesions can become unstable, and if they rupture, they can lead to a heart attack.
We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination. ~ Circulation November 16, 2021
So, based on the levels of these biomarkers, the test gives you a score that predicts your 5-year risk, as a percentage chance, of developing acute coronary syndrome (ACS). Elevated levels raise your PULS score while levels below the norm lower it.
COVID-Jabbed Patients More Than Double Their ACS Risk
According to the authors of the Circulation report:4
“The score has been measured every 3-6 months in our patient population for 8 years. Recently, with the advent of the mRNA COVID 19 vaccines (vac) by Moderna and Pfizer, dramatic changes in the PULS score became apparent in most patients. This report summarizes those results.
A total of 566 [patients], aged 28 to 97, M:F ratio 1:1 seen in a preventive cardiology practice had a new PULS test drawn from 2 to 10 weeks following the 2nd COVID shot and was compared to the previous PULS score drawn 3 to 5 months previously pre- shot.
Baseline IL-16 increased from 35=/-20 above the norm to 82 =/- 75 above the norm post-vac; sFas increased from 22+/- 15 above the norm to 46=/-24 above the norm post-vac; HGF increased from 42+/-12 above the norm to 86+/-31 above the norm post-vac.
These changes resulted in an increase of the PULS score from 11% 5-year ACS risk to 25% 5-year ACS risk. At the time of this report, these changes persist for at least 2.5 months post second dose of vac.
We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.”
As noted by Malhotra, this is indeed extraordinarily disturbing. Patients who received a two-dose regimen of mRNA more than doubled their five-year ACS risk, driving it from an average of 11% to 25%. Just imagine the shape our medical system and society at large will be in if 1 of every 4 people who got the two-dose regimen ends up with acute heart failure.
Signs and Symptoms to Watch For
ACS is an umbrella term that doesn’t just include heart attacks, but also a range of other conditions involving abruptly reduced blood flow to your heart. Signs and symptoms of ACS typically begin very suddenly, and include:5
| Chest pain/discomfort, often described as aching, pressure, tightness or burning sensations | Pain that radiates from your chest to your shoulders, arms, upper abdomen, back, neck and/or jaw |
| Nausea and/or vomiting | Indigestion |
| Shortness of breath | Sudden heavy sweating |
| Lightheadedness, dizziness and/or fainting | Unusual or inexplicable fatigue |
| Restlessness and/or apprehensiveness |
If you suspect ACS, do not drive yourself to the hospital. Call for an ambulance, as it is a true medical emergency that may need prompt medical attention. Risk factors for ACS have historically included older age, high blood pressure, cigarette smoking, lack of exercise, unhealthy diet, excess body weight and diabetes.
SARS-CoV-2 infection was recently added to that list, but it seems we must also add the COVID jab as well. Those who got the injection for fear that COVID-19 might adversely affect their heart now face the grim reality that they’ve exchanged a potential risk for a more certain one.
Vaccine-Induced Thrombocytopenia
In related news, a paper published in the journal Blood Advances reviews “SARS-CoV-2 Spike-Dependent Platelet Activation in COVID-19 Vaccine-Induced Thrombocytopenia.”6 Thrombocytopenia is the medical term for low platelet count.
The authors point out that following the rollout of the mRNA and DNA-based COVID shots, more than 150 cases of thrombocytopenia have been reported. The reference for that statistic is a March 9, 2021, paper in the American Journal of Hematology,7 and injuries are stacking up at breakneck speed.
As of November 12, 2021, there were 4,387 cases of thrombocytopenia reported to the U.S. Vaccine Adverse Events Reporting System (VAERS),8 so it’s far more frequent than what they’re stating. (There are also 9,332 reports of heart attacks, which we just discussed, and 13,237 reports of myopericarditis, i.e., inflammation of the heart and/or heart sack.9)
According to the authors, identifying the mechanism by which the shots cause thrombocytopenia would facilitate the development of a diagnostic test. Historically, heparin-induced thrombocytopenia has been diagnosed using a serotonin release assay (SRA).
Using SRA, a subset of critically ill COVID-19 patients have tested positive for platelet-activating immune complexes that can cause thrombosis. Other researchers have also showed IgG antibodies from critically ill COVID-19 patients can activate platelets, resulting in a thrombotic event.
Here, using a modified SRA, they discovered spike-dependent, platelet-activating immune complexes in a patient with vaccine-induced thrombocytopenia, suggesting the spike protein is the causative factor. They explain:10
“Our patient was a 25-year-old woman who presented to hospital 10 days after receiving the Moderna mRNA COVID-19 vaccine with fatigue, petechiae and wet purpura. The initial platelet count was 1,000 per cubic millimeter without evidence of schistocytes on blood smear.
Coagulation studies were within the normal range … This also likely excludes the presence of a lupus anticoagulant, given the use of a lupus-sensitive reagent for PTT testing. Anti-platelet factor 4 (PF4)/heparin antibodies were not detected … and the classic SRA test, with or without heparin or exogenous PF4, was negative.
Assays for drug-induced immune thrombocytopenia with washed donor platelets were also negative for platelet binding with vaccine, PEG2000, or SARS-CoV-2 Spike protein … The patient was treated with dexamethasone and intravenous immune globulin (IVIg) for a presumed immune thrombocytopenic purpura. The platelet count normalized by day seven of treatment.
Additional serum testing identified SARS-CoV-2 Spike protein antibodies of the IgG … IgA … and IgM … classes. Antibodies against SARS-CoV-2 nucleocapsid protein were absent, confirming vaccine-induced antibodies without prior infection.
To further investigate the mechanism of thrombocytopenia, we tested the patient’s serum using a modified SRA with addition of recombinant SARS-CoV-2 Spike protein (Spike-SRA). We observed dose-dependent platelet activation with increasing SARS-CoV-2 Spike protein …
The reaction was inhibited by an FcγRIIa blocker … and IVIg … confirming FcγRIIa-dependent platelet activation. Platelet activation was also demonstrated to a lesser degree with increasing amounts of Moderna vaccine … and the excipient PEG2000 …
Furthermore, platelet activation was not detected in a control sample from a patient who had received the Moderna vaccine and had not developed thrombocytopenia …
Circulating Spike protein was detected in our patient’s serum using enzyme immunoassay testing … Together, these results suggest that the thrombocytopenia in this patient was secondary to FcγRIIa-mediated platelet activation by SARS-CoV-2 Spike immune complexes.”
Potential Mechanism Identified
If you found the section quoted above to be too complex, here’s the take-home message: The mRNA shot may be causing an exceptionally low level of platelets through a mechanism that involves antibodies against the spike protein (anti-spike antibodies) resulting in depletion of platelets by activating them.
Platelets are specialized cells that stop bleeding, and they have ACE2 receptors, which is what the SARS-CoV-2 spike protein binds to. When the spike protein binds to the ACE2 receptor on the platelets, it activates them.
This platelet activation can lead to disseminated intravascular coagulation, i.e., a pathological overstimulation of your coagulation system that can result in abnormal, and life threatening, blood clotting, as well as thrombocytopenia (low platelet count) and hemorrhaging.
Doctors for COVID Ethics described this mechanism in a February 28, 2021, letter11 to the European Medicines Agency (EMA). In that letter, they warned that, based on this mechanism, spike protein-based COVID shots are likely to cause blood clots, cerebral vein thrombosis and sudden death, which is precisely what we’ve been seeing ever since.
In essence, you basically end up with so many blood clots throughout your vascular system that your coagulation system is exhausted, hence the low platelet count. The low platelet count, in turn, is what allows for hemorrhaging (abnormal bleeding).
Questions Remain
A mystery that remains to be solved is why only certain people with antibodies to the spike protein (anti-spike antibodies) go on to develop symptoms of platelet activation and thrombocytopenia. Why not all of them? “One hypothesis is that platelet activation is dependent on unique spike protein epitopes, which are only recognized by a minority of identified antibodies,” the authors suggest.12 In closing, they state:
“Our case … highlights the applicability of the SRA to detect platelet activation disorders aside from HIT [heparin-induced thrombocytopenia]. Although classically done in the presence of heparin, it can be modified to include various antigens to elicit immune complex formation and identify platelet activation …
Ultimately, the role of SARS-CoV-2 Spike protein requires further clarification in regards to platelet activation, as well as the role of vaccine- and PEG-dependent platelet activation. We postulate that a small subset of antibodies against the Spike protein, formed after vaccination, can activate platelets and cause thrombocytopenia.
The prevalence of this phenomenon remains to be clinically determined. Regardless, the modified SRA presented here may be a useful diagnostic test as more cases of vaccine-induced thrombocytopenia are recognized.”
COVID Jab Risks Clearly Outweigh Any Potential Benefit
Since well before the rollout of these COVID shots, scientists and doctors have sounded the alarm, pointing out a host of potential mechanisms by which they may cause harm. Now, nearly a year into it, many of our fears are turning out to have been warranted. They’re causing very serious cardiovascular damage, blood disorders, and reproductive dysfunction.
Worst of all, our health authorities have abandoned the mandate to protect public health and are covering up the wreckage on behalf of the profit makers. On top of that, doctors and nurses who speak out about the collateral damage they’re seeing are being silenced and persecuted by medical boards and government officials alike.
Now, we’re injecting these kill shots into children as young as 5. I see no way for this to end on a pleasant note. As a society, as the deaths and injuries, especially in children, continue to escalate, we’re going to face some excruciatingly difficult times.
To remind you of where this article started, people who have received two mRNA shots have more than doubled their five-year risk of acute coronary events, on average. If you’ve not yet taken the jab, I reckon you probably won’t at this point. But if you’ve already taken one or two, I strongly urge you to review the mechanisms of harm, and evaluate whether it’s worth it to continue with a third.
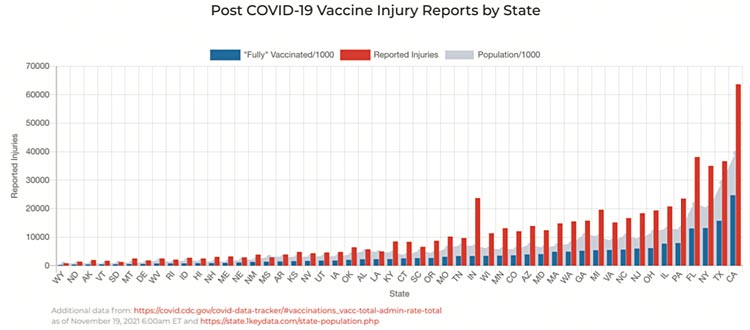
The adverse changes caused by the shots persist for at least 2.5 months. That’s the low end. We still do not know what the upper time limit is. It could be a year or more, and the risks certainly do not diminish with subsequent additional doses. In the November 12, 2021, OpenVAERS report,13 they added a graph showing vaccination rates and VAERS reports by state.
As you can see, there’s a clear correlation between the rate of “fully vaccinated” in a given state and the number of COVID injuries reported from that state. (Indiana, for some reason, sticks out as a lone exception with a disproportionately high number of reports to the number of fully “vaccinated.”)
The gray zones are population; blue bars are the number of fully vaccinated; the red bars are the number of reported injuries. (All numbers have been divided by 1,000.) This is yet another piece of evidence that we have a serious problem on our hands.
What Can You Do if You Have Jab Remorse?
If you now believe that getting the COVID jab was a mistake and wish to lessen your doubled risk of cardiac complications, there a few basic strategies I would advise.
1. Make certain you measure your blood vitamin D level and take enough vitamin D orally (typically about 8,000 units/day for most adults) to make sure your level is 60 to 80 ng/ml (150 to 2000 nmol/l).
2. Eliminate all vegetable (seed) oils in your diet, which involves eliminating nearly all processed foods and most meals in restaurants unless you convince the chef to only cook with butter. Avoid any sauces or salad dressings in restaurants as they are loaded with seed oils. Also avoid chicken and pork as they are very high in linoleic acid, the omega-6 fat that is far too high in nearly everyone and contributes to oxidative stress that causes heart disease.
3. Consider taking around 500 mg/day of NAC, as it helps prevent blood clots and is a precursor for your body to produce the important antioxidant glutathione.
4. Consider fibrinolytic enzymes that digest the fibrin that leads to blood clots, strokes and pulmonary embolisms. The dose is typically two, twice a day, but must be taken on an empty stomach, either an hour before or two hours after a meal. Otherwise, the enzymes will digest your food and not the fibrin in the blood clot.